Kidney Cancer
Kidney cancer is one of the few cancers increasing with incidence in the modern era. More common in men than women, this increase has been linked to aspects of modern society, including obesity and poorly controlled hypertension, as well as to smoking.
The mainstay of treatment for localised kidney cancers is surgical removal and in the vast majority of cases this should involve minimally invasive approaches i.e key hole or laparoscopic surgery or now robotic assisted surgery using the Da Vinci Robot System, rather than open surgery that can result in larger, painful and occasionally disfiguring wounds. However in some cases open surgery remains the best option.
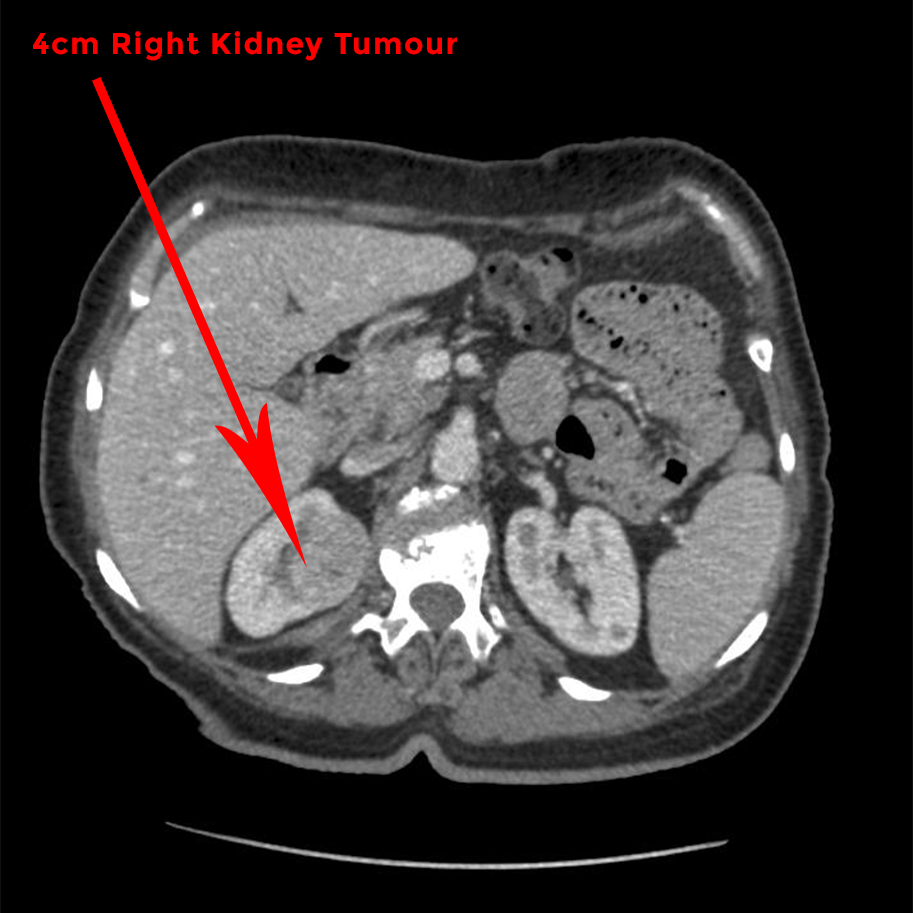
The area of greatest increase in the surgical management of kidney cancer has been that of small (less than 4cm) and medium sized (4-7cm) incidentally discovered tumours, and this is in part due to the greater number of Ultrasound and CT scans now performed, often for other reasons. The vast majority of tumours are therefore found by chance.
For this growing group of patients the aim of surgery is to remove the cancerous tumour with minimum impact upon overall kidney function. This is known as nephron sparing surgery, the nephron being the functioning unit of the kidney. Most often this means a partial nephrectomy (excision of only the tumour mass) although there are other ablative options to kill the tumour e.g cryoablation or freezing of the tumour.
The technical demands of partial nephrectomy have meant that few cases were suitable for a minimally invasive approach and it remains true in the UK that most of these operations are performed through a large wound at open surgery. However, the Da Vinci Robotic System has proven to be an extremely precise and effective alternative, giving patients with kidney cancer the option to decide which type of kidney surgery they would prefer. Where appropriate, a large proportion of cancerous tumours are amenable to be being removed by robotic assisted kidney surgery, meaning the patient not only receives quality cancer surgery, but post-op recovery is much faster; the hospital stay is reduced to just 1 or 2 nights and a return to normal activity, including work, is achievable within 1 to 2 weeks.
Urothelial Carcinoma of the Kidney and Ureter
A less common, but potentially more aggressive form of kidney cancer may arise from the lining of the drainage system of the kidney or indeed from the lining of the tube draining the kidney to the bladder (the ureter). This type of kidney cancer is named after the term cells making up this lining - the urothelium. This type of tumour is also known as transitional cell carcinoma.
Kidney surgery is still the mainstay of initial therapy if the disease remains localised to the urinary tract. The gold standard option involves surgical removal of the entire drainage system to the bladder i.e the kidney and ureter and is called a nephro-ureterectomy.
For smaller, lower risk lesions endoscopic and more local ablative treatments may be employed.
Traditionally a nephro-ureterectomy necessitated 2 large incisions and was a major undertaking for the patient. The advent of laparoscopic/ key hole techniques and now robotic assisted kidney surgery has meant that this procedure can be performed with all the benefits of minimally invasive surgery. Thanks to the improvements in precision and dexterity, those undergoing a robotic assisted nephro-ureterectomy leave hospital after 2 nights or so, usually without a urinary catheter and bag